Chronic diseases account for roughly 74 percent of all deaths worldwide each year, according to the World Health Organization. Yet a large share of these conditions are considered preventable. This sobering reality has pushed healthcare systems, clinicians, and patients alike to look beyond reactive treatment and toward proactive, individualized strategies that address disease risk before it becomes disease itself.
The shift is visible across clinics, research institutions, and wellness platforms. Programs built around precision longevity modules are gaining traction as a structured way to organize preventive care around an individual’s unique biology, habits, and risk profile. Rather than applying a single standard protocol to every patient, these modular approaches slice preventive medicine into targeted components, each addressing a distinct dimension of health.
How Modular Preventive Programs Are Structured
At their core, modular preventive medicine programs work by assembling diagnostic and wellness interventions into flexible units that can be combined, adjusted, or swapped based on individual need. This is a meaningful departure from the one-size-fits-all model that has long dominated primary care.
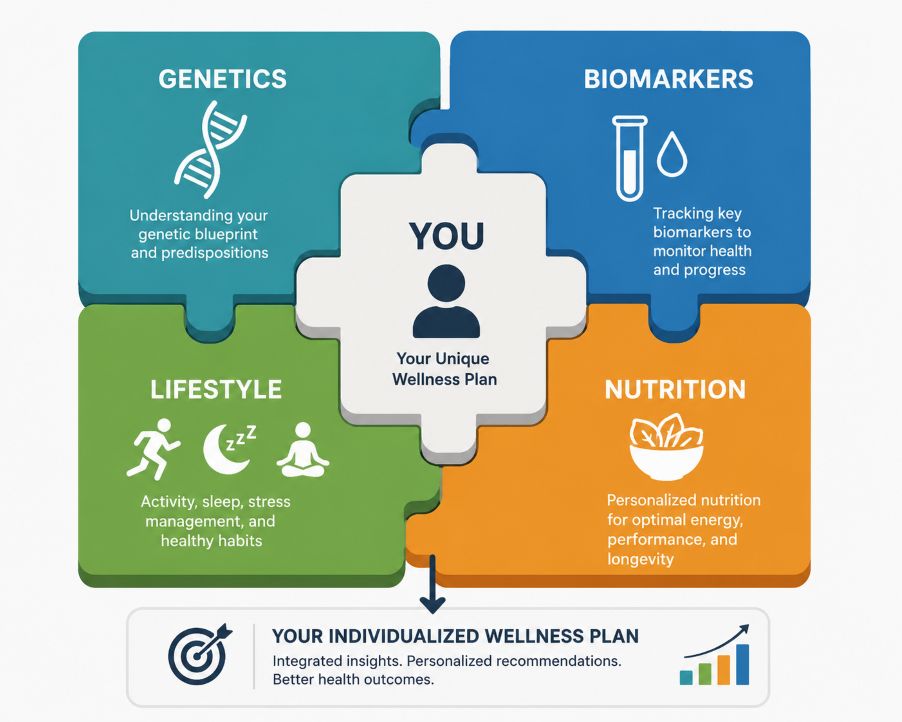
Three main pillars typically inform how these programs are built: biomarker data, genetic analysis, and lifestyle assessment.
Biomarkers serve as the biological baseline. Clinicians measure indicators such as fasting glucose, inflammatory proteins like C-reactive protein, lipid panels, hormone levels, and metabolic markers. Research published in Nature Medicine has demonstrated that biomarker profiles can reveal subclinical disease trajectories years before symptoms appear, giving clinicians a meaningful window for intervention.
Genetic information adds another layer. With the widespread availability of genomic sequencing, practitioners can now identify single nucleotide polymorphisms (SNPs) and other variants that influence how a person metabolizes nutrients, responds to exercise, or processes environmental stressors. The National Institutes of Health has noted that pharmacogenomic and nutrigenomic insights are increasingly being used to tailor preventive recommendations at the individual level.
Lifestyle factors complete the picture. Sleep quality, physical activity patterns, dietary behavior, stress load, and social connection all interact with biological risk in complex ways. Comprehensive intake assessments, validated questionnaires, and wearable device data allow practitioners to quantify these variables and fold them into the overall care design.
The result is a dynamic, patient-specific framework. A middle-aged individual with elevated inflammatory markers, a family history of cardiovascular disease, and a high-stress occupation would receive a very different module configuration than a younger patient with metabolic concerns rooted in dietary patterns and insulin sensitivity. The architecture of each plan reflects the individual, not a demographic average.
The Case For Personalized Preventive Care
Proponents of modular preventive strategies point to several compelling advantages.
First, there is the efficiency argument. By targeting interventions to actual, measured risk, clinicians can avoid both under-treatment and over-treatment. A person with no genetic predisposition to osteoporosis and optimal bone density markers does not need aggressive calcium supplementation or repeated bone scans. Conversely, someone with early signs of metabolic dysfunction can receive intensive dietary and metabolic support before a diabetes diagnosis is warranted.
Second, individualized plans tend to support better patient adherence. Research from the American Journal of Preventive Medicine suggests that patients who understand the specific reasoning behind their care plan are more likely to follow through on recommendations. When someone sees their own biomarker data and understands which lifestyle change addresses which risk factor, the recommendations carry more personal weight.
Third, modular frameworks are adaptable over time. As a patient’s biology changes, as new diagnostic tools emerge, or as the evidence base evolves, individual modules can be updated without redesigning the entire care structure. This flexibility is particularly valuable across the lifespan, where health priorities shift considerably from one decade to the next.
Limitations and Honest Concerns
A dialectical review of this approach requires acknowledging real limitations alongside the promise.
Cost and access remain serious barriers. Comprehensive genomic sequencing, advanced biomarker panels, and ongoing specialist oversight are expensive. Data from the Kaiser Family Foundation consistently shows that the patients who might benefit most from preventive investment often have the least access to it. Without deliberate effort to integrate modular preventive programs into insurance structures and community health settings, these approaches risk deepening existing health inequities.
There is also the issue of evidence maturity. While the scientific rationale for precision-based prevention is sound, long-term outcome data for many specific modular protocols is still accumulating. Experts at the Preventive Medicine Research Institute caution that enthusiasm for novel biomarkers and genetic tools should be tempered by rigorous clinical validation. Not every measurable variable is an actionable one, and confusing the two can lead to unnecessary anxiety or harmful over-intervention.
Data privacy is another legitimate concern. Genetic and biomarker data is among the most sensitive health information a person can generate. Questions about how this data is stored, who has access to it, and how it may be used in insurance or employment contexts are not yet fully resolved in most regulatory frameworks.
Finally, the integration challenge is real. For modular programs to work effectively within broader healthcare systems, they require coordination across primary care, specialty medicine, laboratory services, and digital health platforms. In fragmented health systems, achieving that coordination consistently is difficult.
The Future of Individualized Treatment Planning
Despite these challenges, the trajectory of preventive medicine is clearly moving toward greater personalization. Advances in artificial intelligence and machine learning are accelerating the ability to synthesize complex, multi-variable patient data into actionable clinical insights. The Harvard T.H. Chan School of Public Health has highlighted machine learning models that can predict cardiometabolic risk with greater precision than traditional scoring tools by incorporating a wider range of individual data points. This momentum extends beyond physical health, with advances in personalized psychiatric treatment now drawing on similar genetic and AI-driven frameworks to improve mental health outcomes at the individual level.
At the same time, the cost of genomic and biomarker testing continues to fall. Tools that were once available only in research settings are increasingly accessible in clinical practice, and some are beginning to reach consumers directly. This democratization of data, if paired with appropriate clinical guidance, could meaningfully broaden access to tailored preventive planning.
Regulatory bodies are also beginning to catch up. The U.S. Food and Drug Administration has been developing clearer frameworks for evaluating digital health tools and laboratory-developed tests, which should eventually give both clinicians and patients greater confidence in the validity of the tools that inform these individualized programs.
The shift from population-level prevention toward patient-specific wellness architecture is not a rejection of public health principles. It is an evolution of them. When individualized preventive care plans are built on rigorous evidence, structured equitably, and integrated thoughtfully into existing systems, they hold genuine potential to reduce the burden of chronic disease in ways that broad, undifferentiated protocols simply cannot achieve.
The modular approach to preventive health is not a finished product. It is a framework in active development, one that invites both optimism and critical scrutiny. The medical community’s challenge is to refine it honestly, ensuring that personalized longevity planning becomes a tool for better outcomes across populations, not merely a premium service for the few.